For much of the past year, life in Western Australia has been coronavirus-free. Friends gathered in pubs; people kissed and hugged their relatives; children went to school without temperature checks or wearing masks. The state maintained this enviable position only by placing heavy restrictions on travel and imposing lockdowns — some regions entered a snap lockdown at the beginning of the year after a security guard at a hotel where visitors were quarantined tested positive for the virus. But the experience in Western Australia has provided a glimpse into a life free from the SARS-CoV-2 coronavirus. If other regions, aided by vaccines, aimed for a similar zero-COVID strategy, then could the world hope to rid itself of the virus?
It’s a beautiful dream but most scientists think it’s improbable. In January, Nature asked more than 100 immunologists, infectious-disease researchers and virologists working on the coronavirus whether it could be eradicated. Almost 90% of respondents think that the coronavirus will become endemic — meaning that it will continue to circulate in pockets of the global population for years to come (see 'Endemic future').
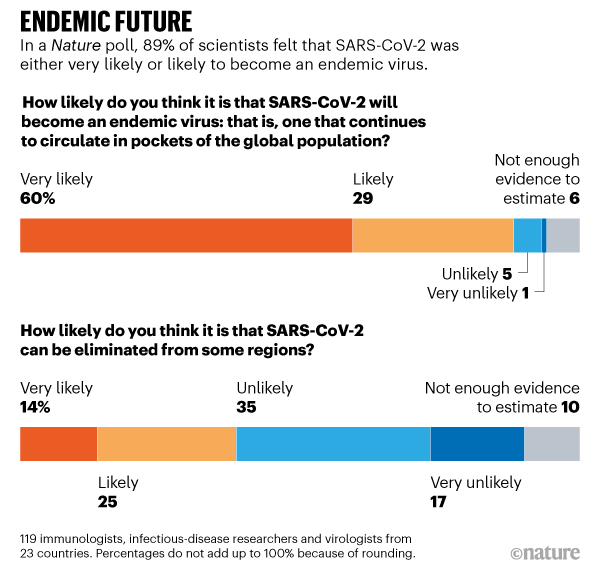
Source: Nature survey
“Eradicating this virus right now from the world is a lot like trying to plan the construction of a stepping-stone pathway to the Moon. It’s unrealistic,” says Michael Osterholm, an epidemiologist at the University of Minnesota in Minneapolis.
But failure to eradicate the virus does not mean that death, illness or social isolation will continue on the scales seen so far. The future will depend heavily on the type of immunity people acquire through infection or vaccination and how the virus evolves. Influenza and the four human coronaviruses that cause common colds are also endemic: but a combination of annual vaccines and acquired immunity means that societies tolerate the seasonal deaths and illnesses they bring without requiring lockdowns, masks and social distancing.
More than one-third of the respondents to Nature’s survey thought that it would be possible to eliminate SARS-CoV-2 from some regions while it continued to circulate in others. In zero-COVID regions there would be a continual risk of disease outbreaks, but they could be quenched quickly by herd immunity if most people had been vaccinated. “I guess COVID will be eliminated from some countries, but with a continuing (and maybe seasonal) risk of reintroduction from places where vaccine coverage and public-health measures have not been good enough,” says Christopher Dye, an epidemiologist at the University of Oxford, UK.
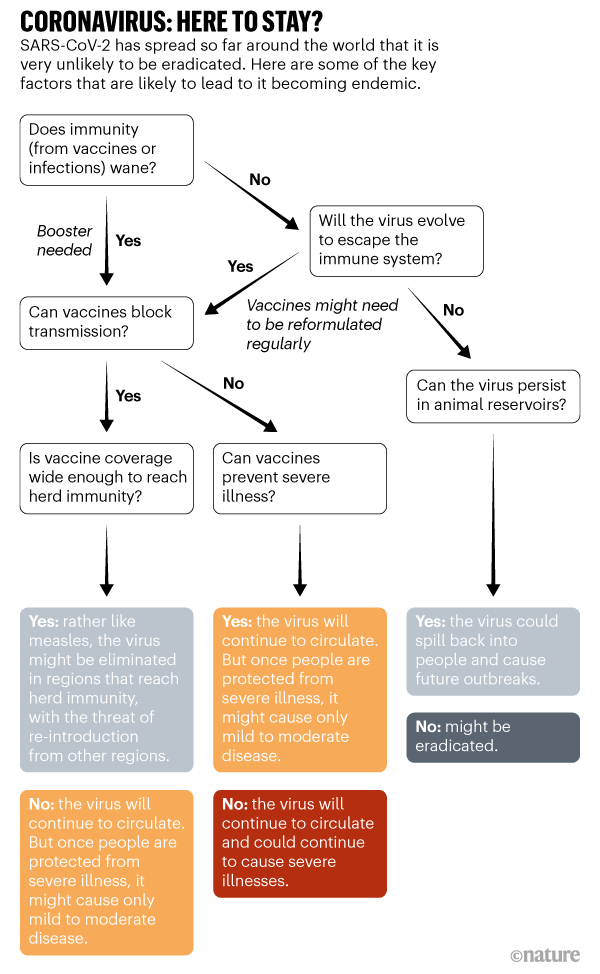
“The virus becoming endemic is likely, but the pattern that it will take is hard to predict,” says Angela Rasmussen, a virologist from Georgetown University, who is based in Seattle, Washington. This will determine the societal costs of SARS-CoV-2 for 5, 10 or even 50 years in the future (see ‘Coronavirus: here to stay?’).
Childhood virus
Five years from now, when childcare centres call parents to tell them that their child has a runny nose and a fever, the COVID-19 pandemic might seem a distant memory. But there’s a chance the virus that killed more than 1.5 million people in 2020 alone will be the culprit.
This is one scenario that scientists foresee for SARS-CoV-2. The virus sticks around, but once people develop some immunity to it — either through natural infection or vaccination — they won’t come down with severe symptoms. The virus would become a foe first encountered in early childhood, when it typically causes mild infection or none at all, says Jennie Lavine, an infectious-disease researcher at Emory University in Atlanta, Georgia.
Scientists consider this possible because that’s how the four endemic coronaviruses, called OC43, 229E, NL63 and HKU1, behave. At least three of these viruses have probably been circulating in human populations for hundreds of years; two of them are responsible for roughly 15% of respiratory infections. Using data from previous studies, Lavine and her colleagues developed a model that shows how most children first come down with these viruses before the age of 6 and develop immunity to them1. That defence wanes pretty quickly so it is not sufficient to block reinfection entirely, but it seems to protect adults from getting sick, says Lavine. Even in children, the first infection is relatively mild.
Whether immunity to SARS-CoV-2 will behave in the same way is so far unclear. A large study of people who have had COVID-19 suggests that their levels of neutralizing antibodies — which help to block reinfection — start to decline after around six to eight months2. But their bodies also make memory B cells, which can manufacture antibodies if a new infection arises, and T cells that can eliminate virus-infected cells, says Daniela Weiskopf, an immunologist at the La Jolla Institute for Immunology in California, who co-authored the study. It’s yet to be established if this immune memory can block viral reinfection — although cases of reinfection have been recorded, and new viral variants might make them more likely, they are still considered rare.
Weiskopf and her colleagues are still tracking the immune memory of people infected with COVID-19 to see if it persists. If most people develop life-long immunity to the virus, either through natural infection or vaccination, then the virus is unlikely to become endemic, she says. But immunity might wane after a year or two — and already there are hints that the virus can evolve to escape it. More than half the scientists who responded to Nature’s survey think waning immunity will be one of the main drivers of the virus becoming endemic.
Because the virus has spread around the world, it might seem that it could already be classed as endemic. But because infections continue to increase worldwide, and with so many people still susceptible, scientists still technically class it as in a pandemic phase. In the endemic phase, the number of infections becomes relatively constant across years, allowing for occasional flare-ups, says Lavine.
To reach this steady state could take a few years or decades, depending on how quickly populations develop immunity, says Lavine. Allowing the virus to spread unchecked would be the fastest way to get to that point — but that would result in many millions of deaths. “That path has some huge costs,” she says. The most palatable path is through vaccination.
Vaccines and herd immunity
Countries that have begun distributing COVID-19 vaccines soon expect to see a reduction in severe illness. But it will take longer to see how effectively vaccines can reduce transmission. Data from clinical trials suggest that vaccines that prevent symptomatic infection might also stop a person from passing on the virus.
If vaccines do block transmission — and if they remain effective against newer variants of the virus — it might be possible to eliminate the virus in regions where enough people are vaccinated so that they can protect those who are not, contributing to herd immunity. A vaccine that is 90% effective at blocking transmission will need to reach at least 55% of the population to achieve temporary herd immunity as long as some social distancing measures — such as face masks and many people working from home — remain in place to keep transmission in check, according to a model3 developed by Alexandra Hogan at Imperial College London and her colleagues. (A vaccine would need to reach almost 67% of people to provide herd immunity if all social distancing measures were lifted.) But if the rate of transmission increases because of a new variant, or if a vaccine is less effective than 90% at blocking transmission, vaccine coverage will need to be greater to blunt circulation.
Vaccinating even 55% of the population will be challenging in many countries. “The virus will stick around if parts of the world don’t get vaccinated,” says Jeffrey Shaman, an infectious-disease researcher at Columbia University in New York City.
Even if the virus remains endemic in many regions, global travel will probably resume when severe infections are reduced to levels that health services can cope with, and when a high proportion of people who are vulnerable to severe illness have been vaccinated, says Dye.
Similar to flu?
The 1918 influenza pandemic, which killed more than 50 million people, is the yardstick by which all other pandemics are measured. It was sparked by a type of virus known as influenza A, which originated in birds. Almost all cases of influenza A since then, and all subsequent flu pandemics, have been caused by descendants of the 1918 virus. These descendants circulate the globe, infecting millions of people each year. Flu pandemics occur when populations are naive to a virus; by the time a pandemic virus becomes seasonal, much of the population has some immunity to it. Seasonal flu still has a significant toll globally, claiming roughly 650,000 lives per year.
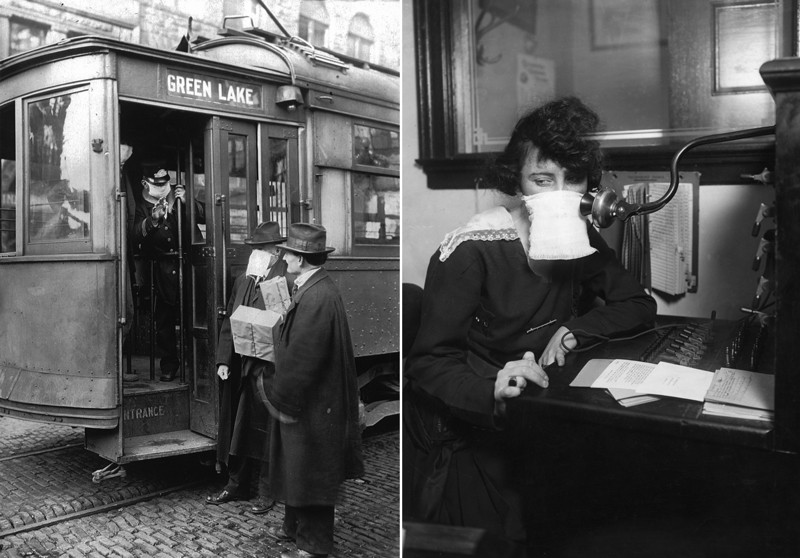
US commuters and telephone operators wore face masks in the 1918 influenza pandemic.Credit: PhotoQuest/Getty; Bettmann/Getty
Jesse Bloom, an evolutionary biologist at the Fred Hutchinson Cancer Research Center in Seattle, thinks the coronavirus might follow a similar path. “I do think SARS-CoV-2 will become a less serious problem and something like flu,” he says. Shaman and others say the virus could also settle into a seasonal pattern of annual winter outbreaks similar to flu.
Flu seems to evolve much faster than SARS-CoV-2, allowing it to sneak past the immune system’s defences. This feature is why flu vaccines need to be reformulated each year; that might not be needed for SARS-CoV-2.
Still, the coronavirus might be able to dodge immunity acquired by infection, and possibly outsmart vaccines. Already, laboratory studies show that neutralizing antibodies in the blood of people who have had COVID-19 are less capable of recognizing a viral variant first identified in South Africa (called 501Y.V2), than variants that circulated earlier in the pandemic4. That is probably because of mutations in the virus’s spike protein, which vaccines target. Trial results suggest that some vaccines might be less effective against 501Y.V2 than against other variants, and some vaccine makers are exploring redesigns of their products.
Still, the immune system has lots of tricks up its sleeve, and can respond to many features of the virus, not just spike, says Lavine. “The virus is probably going to have to go through lots of mutations to make a vaccine ineffective,” she says. Preliminary trial results also suggest that vaccines can protect people with 501Y.V2 against severe disease, says Rasmussen.
More than 70% of the researchers surveyed by Nature think that immune escape will be another driver of the virus’s continuing circulation (see 'Driving factors'). This would not be a first for a human coronavirus. In a study5 yet to be peer reviewed, Bloom and his colleagues show that the endemic coronavirus 229E has evolved so that neutralizing antibodies in the blood of people infected with the viral variant circulating in the late 1980s and early 1990s are much less effective against more recent variants. People are reinfected with 229E over their lifetime, and Bloom suspects that it might be harder to stave off the variants that have evolved to escape previous immunity. But scientists don’t know whether these reinfections are associated with worse symptoms. “I would expect that over many years, accumulated mutations to SARS-CoV-2 will more completely erode neutralizing antibody immunity as we saw for CoV-229E, although I can’t say for sure how the rates will compare among the two coronaviruses,” says Bloom.
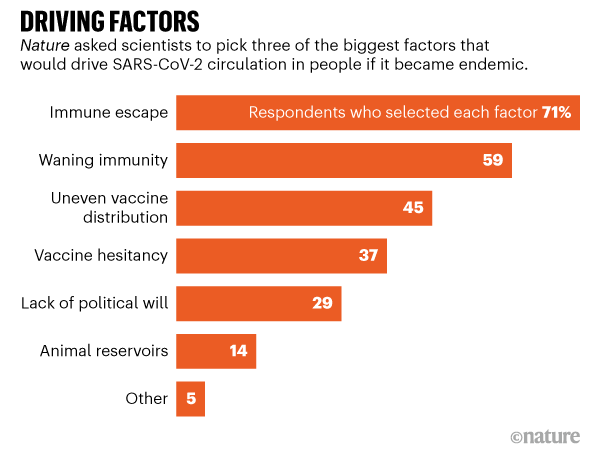
Source: Nature survey
Bloom thinks it’s probable that SARS-CoV-2 vaccines will need to be updated, possibly every year. But even then, immunity from either past vaccination or infection will probably blunt serious disease, he says. And Lavine notes that even if people are reinfected, this might not be a big deal. With the endemic coronaviruses, frequent reinfections seem to boost immunity against related variants and typically people experience only mild symptoms, she says. But it is possible that vaccines won’t stop some people developing severe symptoms, in which case the virus will continue to be a significant burden on society, says Shaman.
Measles-like virus
If SARS-CoV-2 vaccines block infection and transmission for life, the virus might become something akin to measles. “It’s probably less likely [than other scenarios] but it’s still possible,” says Shaman.
With a highly effective measles vaccine — two doses and a person is protected for life — the measles virus has been eliminated in many parts of the world. Before a vaccine was developed in 1963, major epidemics killed about 2.6 million people, mostly children, a year. Unlike flu vaccines, the immunization for measles has never needed to be updated because the virus has yet to evolve in ways that evade the immune system.
Measles is still endemic in parts of the world with insufficient immunization. In 2018, a global resurgence killed more than 140,000 people. A similar situation could emerge with SARS-CoV-2 if people decline vaccines. A survey of more than 1,600 US citizens found that more than one-quarter would definitely or probably decline a COVID-19 vaccine, even if it were free and deemed safe (see go.nature.com/3a9b44s). “How successful we are at addressing those concerns will determine how many people get the vaccine and how many remain susceptible,” says Rasmussen.
Animal reservoirs
The future of SARS-CoV-2 will also depend on whether it establishes itself in a wild animal population. Several diseases brought under control persist because animal reservoirs, such as insects, provide chances for pathogens to spill back into people. These include yellow fever, Ebola and chikungunya virus.
SARS-CoV-2 probably originated in bats, but it might have passed to people through an intermediate host. The virus can readily infect many animals, including cats, rabbits and hamsters. It is particularly infectious in mink, and mass outbreaks on mink farms in Denmark and the Netherlands have led to huge animal culls. The virus has also passed between minks and people. If it became established in a wild-animal population and could spill back into people, it would be very difficult to control, says Osterholm. “There is no disease in the history of humankind that has disappeared from the face of the Earth when zoonotic disease was such an important part of, or played a role in, the transmission,” he says.
The path that SARS-CoV-2 might take to become an endemic virus is challenging to predict, but society does have some control over it. In the next year or two, countries can reduce transmission with control measures until enough people have been vaccinated either to achieve herd immunity or to drastically reduce the severity of infections. That would significantly reduce deaths and severe disease, says Osterholm. But if countries abandon strategies to reduce spread and let the virus reign unchecked then “the darkest days of the pandemic are still ahead of us”, he says.
"Here" - Google News
February 16, 2021 at 05:10PM
https://ift.tt/3aoV96T
The coronavirus is here to stay — here's what that means - Nature.com
"Here" - Google News
https://ift.tt/39D7kKR
Shoes Man Tutorial
Pos News Update
Meme Update
Korean Entertainment News
Japan News Update
:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/25244079/4.png)



No comments:
Post a Comment